Assessment - Disabled by the Discourse Thesis
I kept coming back to the same question. What is the purpose of the assessment and what value is it adding? I particularly liked the way that the parents refused to allow the MRI as it was not going to add anything and, in fact, it may subtract for Maggie's life experiences as it may act to limit what people try in order to provide education for her and to teach her the skills (she's never going to be able to do this so why should we bother trying to teach it to her).
Reflections on pages 196-227 using the prompts from the first booklet.
a) What this reading highlighted for you. Consider for example, the language that is used to describe Maggie-Rose, the extent to which the family were consulted about their perspective, the types of assessments that were conducted, the questions that were asked of the family, and the focus and purpose behind the assessment.
This reading highlighted the stark difference between a medical and social model. The family's thoughts and processes were firmly a social model. The social model says that it is society's role to remove any barriers and the individual is the expert on their requirements. In this case, until Maggie reached an age where she could speak for herself, her parents were the experts on her behalf and they advocated for her. They were attuned to her needs and could read her really well. There didn't seem to be much consultation and the way the 'experts' worked didn't fit into the He Ritenga Whaimōhio model. In fact, they seemed to completely come from a medical model and they viewed Maggie as needing a diagnosis. I was shocked about them wanting to do and MRI to see if it could show whether she might develop language. I applauded the parents questioning whether it was necessary and what value would it add. No value would be added so it was good that they refused it and just carried on with raising their daughter.
I was in agreement with how they responded to EIS assessments in that they only allowed them with prior consent. I was again shocked to hear that they conduct assessments without the parents being aware.
This reading highlighted the stark difference between a medical and social model. The family's thoughts and processes were firmly a social model. The social model says that it is society's role to remove any barriers and the individual is the expert on their requirements. In this case, until Maggie reached an age where she could speak for herself, her parents were the experts on her behalf and they advocated for her. They were attuned to her needs and could read her really well. There didn't seem to be much consultation and the way the 'experts' worked didn't fit into the He Ritenga Whaimōhio model. In fact, they seemed to completely come from a medical model and they viewed Maggie as needing a diagnosis. I was shocked about them wanting to do and MRI to see if it could show whether she might develop language. I applauded the parents questioning whether it was necessary and what value would it add. No value would be added so it was good that they refused it and just carried on with raising their daughter.
I was in agreement with how they responded to EIS assessments in that they only allowed them with prior consent. I was again shocked to hear that they conduct assessments without the parents being aware.
b) The implications of this information for your own assessment practice.
I need to think really carefully about what tests/assessments I am doing on a student and what purpose it serves. I have always been wary about 'labelleing' and the purpose of putting a label on to a student. There needs to be a clear reason for a label and it needs to not be an excuse. I remember having a conversation with a SENCo about a student. I asked if they had an idea of what was driving the behaviour. The answer was 'They're ADD.' (They HAVE ADD, not ARE ADD). My response was 'Yes, that is the diagnosis, but what drives the behaviour, what is the motivation?' they seemed a bit taken aback. The diagnosis explained the behaviour in their mind. I had to explain that the behaviour can still be driven by other factors. What I was wanting was for them to change their lens and look at all the factors that drives behaviour and not just blame it on the diagnosis. I was inadvertently employing a social model.
I have been guilty of doing assessment for the sake of doing assessment. I believe that at my previous school I over-assessed and gave unnecessary assessments because I had to tick the boxes. We put our students through a barrage of assessments and didn't trust the previous schools' data. We did have a look at the old data and compared it with our new data and there was a mis-match so I guess that was why we didn't trust the old data. I would have loved to have been able to put the questions out there of why are we doing all this assessment, but I wasn't in the place to do so. I also knew there was too much assessment when I ran out of lines to put all my data in when filling in a form for Northern Health School.
The example I have for assessment for the wrong reasons comes from the dark days of 'National Standards' when we were moderating asTTLe writing samples. One team member asked us our opinion on whether something was a 2 or 3. The other team member immediately answered 'It's the beginning of the year, it's a 2' without even looking at the piece of work. I also used to teach paragraphing as I knew that was weighted quite heavily in the marking scheme and that way I would 'demonstrate progress'. I also read the writing of another class. The writing was very flowery and formulaic and pretty much the same. We were all guilty of trying to skew the final assessment data to make ourselves look better.
I need to think really carefully about what tests/assessments I am doing on a student and what purpose it serves. I have always been wary about 'labelleing' and the purpose of putting a label on to a student. There needs to be a clear reason for a label and it needs to not be an excuse. I remember having a conversation with a SENCo about a student. I asked if they had an idea of what was driving the behaviour. The answer was 'They're ADD.' (They HAVE ADD, not ARE ADD). My response was 'Yes, that is the diagnosis, but what drives the behaviour, what is the motivation?' they seemed a bit taken aback. The diagnosis explained the behaviour in their mind. I had to explain that the behaviour can still be driven by other factors. What I was wanting was for them to change their lens and look at all the factors that drives behaviour and not just blame it on the diagnosis. I was inadvertently employing a social model.
I have been guilty of doing assessment for the sake of doing assessment. I believe that at my previous school I over-assessed and gave unnecessary assessments because I had to tick the boxes. We put our students through a barrage of assessments and didn't trust the previous schools' data. We did have a look at the old data and compared it with our new data and there was a mis-match so I guess that was why we didn't trust the old data. I would have loved to have been able to put the questions out there of why are we doing all this assessment, but I wasn't in the place to do so. I also knew there was too much assessment when I ran out of lines to put all my data in when filling in a form for Northern Health School.
The example I have for assessment for the wrong reasons comes from the dark days of 'National Standards' when we were moderating asTTLe writing samples. One team member asked us our opinion on whether something was a 2 or 3. The other team member immediately answered 'It's the beginning of the year, it's a 2' without even looking at the piece of work. I also used to teach paragraphing as I knew that was weighted quite heavily in the marking scheme and that way I would 'demonstrate progress'. I also read the writing of another class. The writing was very flowery and formulaic and pretty much the same. We were all guilty of trying to skew the final assessment data to make ourselves look better.
c) If you were to receive a description of Maggie-Rose based on these contrasting narratives, how this may impact upon your expectations, understanding of, and interactions with Maggie-Rose.
I would like to think that I listened to the parents' narrative and gave that a bit more weight. I think I have always done that in my practice as I would never look at information from contributing schools unless I had a really good reason to (something raised it's head that I was puzzled about or there was relevant diagnostic or learning information). This was vindicated quite early in my teaching career when I had a student labelled as a D3 (low academic and not very well behaved) by their primary school. This student was elected Student Councillor in their first year at Intermediate. They asked me to tell their parents this as their parents didn't believe their child was a class leader and was elected to that position by their peers. It seemed that they were a 'naughty' child who didn't achieve very well academically. I only responded to the child I saw in front of me and hadn't allowed the previous school's information to colour how I interacted with the child. And that seemed to be a really good decision as the student flourished and had made a true fresh start.
I would like to think that I listened to the parents' narrative and gave that a bit more weight. I think I have always done that in my practice as I would never look at information from contributing schools unless I had a really good reason to (something raised it's head that I was puzzled about or there was relevant diagnostic or learning information). This was vindicated quite early in my teaching career when I had a student labelled as a D3 (low academic and not very well behaved) by their primary school. This student was elected Student Councillor in their first year at Intermediate. They asked me to tell their parents this as their parents didn't believe their child was a class leader and was elected to that position by their peers. It seemed that they were a 'naughty' child who didn't achieve very well academically. I only responded to the child I saw in front of me and hadn't allowed the previous school's information to colour how I interacted with the child. And that seemed to be a really good decision as the student flourished and had made a true fresh start.
Links to literature:
Brisenden - when defining the lens that the parents are using to relate to Maggie and her abilities. They see her as not needing a cure as she isn't damaged. This differs from the medical model where they wanted to test and assess in order to come up with a diagnosis that could lead to a prognosis. It was great that the parents questioned the validity of any testing.
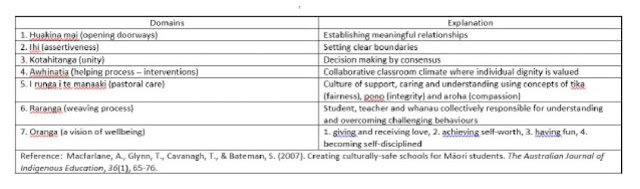
He Ritenga Whaimōhio - when the parents consulted with a team to work together to support Maggie, the team came to their home (as opposed to them travelling to meet people). This helps to create the intersection that is He Ritenga Whaimōhio as it draws from the Aroha and Pono sections. Aroha, as the culture of Maggie and her family is acknowledged by them meeting in a space that they are comfortable in. Pono, as Maggie and her family are part of the process.
References:
Brisenden, S. (1986). Independent living and the medical model of disability. Disability, Handicap & Society, 1(2), 173-178.
Macartney, B. C. (2011). Disabled by the discourse: Two families’ narratives of inclusion, exclusion and resistance in education.
Macfarlane, A., & Macfarlane, S. (2014, October 4). He ritenga whaimohio. http://celebratingnorthlandstamariki.co.nz/images/2014/He%20ritenga%20whaim%C5%8Dhio_%20Culturally%20responsive%20pedagogy.pdf
Comments
Post a Comment